Editor’s Note: Trigger Warning. We began developing this story a year ago and, while we stand by the content, be aware that we discuss actual traumatic events including death, child abuse, child sexual assault and sex trafficking, and domestic violence, which may be triggering for some readers. Given the incredibly violent spate of recent shootings – from El Paso to Dayton – ongoing community violence across our nation, and the continued police killings of specifically young Black men, please practice self care while reading this important article on trauma. Edited to clarify some areas of the Flagstaff Academy section.
About the author: Julia Wild has an M.S. Psychology and is a trauma expert.
The Reality of American Trauma
As I read about the gruesome death of 12-year old Eduardo Posso, I couldn’t help but wonder if the shock gripping my chest felt anything like the shock from the dog collar he died wearing. Or the agony of being starved and chained in a bathroom by his own father. Was Eduardo’s agony like the agony that drove 14-year-old Nakia Vanant’s Facebook live suicide in 2017? It was precipitated by her destabilizing transience through fourteen foster homes and her mother’s cutting rejection. Failed by every safe-guard, Nakia and Eduardo share a thread of abuse and trauma that were repeatedly overlooked. Deaths such as theirs are unacceptable. My background in psychology didn’t cushion the impact of reading about them, nor would I want it to. It is important we are not desensitized to their suffering, because being with our own pain is part of the solution to helping children. If their stories point to anything, it is that we need more sensitivity and consciousness when it comes to trauma, not less. Not solely in relation to children, but also adults. What remains unconscious and unhealed within ourselves will be projected upon – and inherited by – our children.
Trauma is America’s silent epidemic. It costs us a growing number of children’s lives. The word trauma comes from the Greek word for “wound.” In 2013, the American Psychiatric Association (APA) released the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5). It was the first time the DSM included a subtype for Post-Traumatic Stress Disorder (PTSD) in children under six years old. This is based on recent findings for the unique presentation of PTSD in young children, and increased prevalence. In the DSM-5, for adults and children over age six, trauma is defined as the following:
Exposure to actual or threatened death, serious injury, or sexual violence in one (or more) of the following ways:
1. Directly experiencing the traumatic event(s).
2. Witnessing, in person, the event(s) as it occurred to others.
3. Learning that the traumatic event(s) occurred to a close family member or close friend. In cases of actual or threatened death of family member or friend, the event(s) must have been violent or accidental.
4. Experiencing repeated or extreme exposure to aversive details of the traumatic event(s) (e.g., first responders collecting human remains; police officers repeatedly exposed to details of child abuse).
Note: Criterion 4A does not apply to exposure through electronic media, television, movies, or pictures, unless this exposure is work related.
For young children under age 6, the definition of trauma is:
Exposure to actual or threatened death, serious injury, or sexual violence in on (or more) of the following ways:
1. Directly experiencing the traumatic event(s).
2. Witnessing, in person, the event(s) as they occurred to others, especially primary caregivers. Note: Witnessing does not include events that are witnessed only in electronic media, television, movies, or pictures.
3. Learning that the traumatic event(s) occurred to a parent or caregiving figure.
 The APA’s definition predominates in institutions today, but such definitions often miss what’s emotionally and spiritually obvious. So much so that Dr. Bessel van der Kolk – a Dutch psychiatrist, author and educator focused on post-traumatic stress, based in Boston, according to wikipedia – observed that up to 82% of traumatized children did not meet criteria for PTSD in his National Child Traumatic Stress Network (2015). Extrapolating this to the general population, it suggests PTSD is immensely underdiagnosed. Depression, ADHD, oppositional defiant disorder, anxiety and other diagnoses can be given instead. In addition, our understanding of healing and what it means to be human are rapidly evolving. It would be myopic to discount other trauma perspectives. For example, from a Shamanic perspective, trauma is seen as a splintering-off of soul fragments which can be retrieved and re-integrated (Harner, 1990). Another perspective, the theory of “epigenetics,” says trauma is inherited via DNA.
The APA’s definition predominates in institutions today, but such definitions often miss what’s emotionally and spiritually obvious. So much so that Dr. Bessel van der Kolk – a Dutch psychiatrist, author and educator focused on post-traumatic stress, based in Boston, according to wikipedia – observed that up to 82% of traumatized children did not meet criteria for PTSD in his National Child Traumatic Stress Network (2015). Extrapolating this to the general population, it suggests PTSD is immensely underdiagnosed. Depression, ADHD, oppositional defiant disorder, anxiety and other diagnoses can be given instead. In addition, our understanding of healing and what it means to be human are rapidly evolving. It would be myopic to discount other trauma perspectives. For example, from a Shamanic perspective, trauma is seen as a splintering-off of soul fragments which can be retrieved and re-integrated (Harner, 1990). Another perspective, the theory of “epigenetics,” says trauma is inherited via DNA.
The DSM-5 describes trauma as an event, without explaining the root cause of traumatic symptoms. Physiologically, traumatic symptoms are caused when the energy of responses that are not completed or discharged become stuck and frozen in the nervous system (Levine, 1997). We will return to this after looking at national and Colorado statistics on child trauma.
 National Child Trauma Statistics
National Child Trauma Statistics
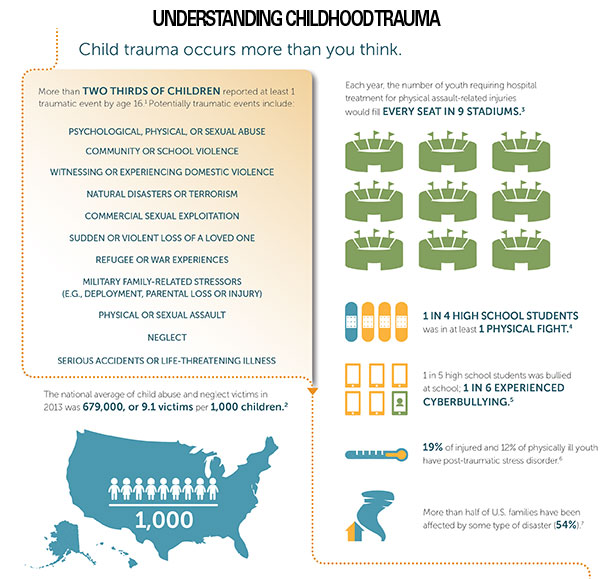
According to the Substance Abuse and Mental Health Services Administration (SAMHSA) (2015), 66.6% of children reported at least one traumatic event by the age of 16 (see infographic). Child abuse and neglect rates then were 9.1 victims per 1,000 children. Just four years later in 2019, the Centers for Disease Control (CDC) released much higher numbers, reporting about one in seven children. The CDC’s findings connect child maltreatment with disrupted neurodevelopment, social/emotional/cognitive impairment, high-risk behaviors, disease and early death.
Their report included economic costs associated with child abuse, estimated at $124 billion in 2008. This rivaled costs of other well-known public health issues, such as type 2 diabetes and stroke. However, a study with wider analysis factors, such as criminal justice costs, reported costs up to $585 billion (Fang et al., 2011). Supporting the link between childhood abuse/neglect and increased criminal justice costs, in 1999 the U.S. Department of Justice (DOJ) compared reported childhood abuse by State and Federal inmates and probationers. Up to 57% of female inmates and 16.4% of male inmates reported childhood abuse by one or both parents – over twice the frequency seen in the general population at the time. 86.7% of state inmate females and 43.6% of state inmate males, who had been in foster care, reported childhood abuse in their foster families. This paints a crushing picture of the abuse Nakia Vanant most likely accumulated in her stay through 14 foster homes.
The Adverse Childhood Experiences Study (1998) found a direct correlation between childhood abuse and leading causes of death, including alcoholism, depression, heart disease, lung disease, cancer and suicide attempts. These staggering findings speak to trauma’s pervasive presence and impact.
 Colorado Child Trauma Statistics
Colorado Child Trauma Statistics
According to a 2018 report from the CDC, Colorado’s teen suicide rate is nearly twice the national average. In teenagers ages 15-19, the suicide rate for the U.S. is 8.9 out of 100,000, compared to 17.6 out of 100,000 in Colorado. Attorney General Cynthia Coffman has called suicide a public health crisis, and acknowledged an alarming youth suicide trend: Between 2015 and 2017, there were 222 suicide deaths of youth ages 10-18. Suicide is the number one cause of death in individuals between 10-34. In what may be a feedback loop, trauma contributes to increased suicidality, which, in turn, may leave communities feeling additionally traumatized, compiling risk for suicidality.
While numbers related to youth suicide in Colorado have increased, child trafficking numbers in Colorado have slightly decreased. Colorado had 22 reported cases of child trafficking, down from 28 in 2017 and 24 in 2016. The Child Abuse and Neglect Hotline reported a record 221,969 calls in 2018, compared to 211,554 in 2017. Social services agencies found 13,289 children experienced abuse or neglect. According to Colorado Children’s Campaign, child abuse rates in 2017 were 9.2 per 1,000 children, compared to 8.4 in 2016 and 7.8 in 2015. Remember that child abuse across all categories are often significantly under-reported.
Boulder County’s rate of reported abuse in 2017 was 4.5 in 1000 children, which is substantially lower than the state average. See related infographics for more detailed data. Before looking at schools, let’s clarify trauma’s impact on a developing child.
Two Key Concepts in Developmental Trauma, Relational Trauma & Fight Flight Freeze
“Relational trauma” is a type of developmental trauma. It underpins most developmental trauma. Laurence Heller, PhD, and Aline LaPierre, PsyD, founded the NeuroAffective Relational Model (NARM), which is specifically for developmental trauma. They define relational trauma as traumatic disruptions in the attachment between child and primary caregivers (2012). Healthy attachment by primary caregivers is foundational in more ways than many realize. Despite similar physiology, the dynamics of relational trauma differentiate it from incidental trauma. In fact, Dr. van der Kolk calls attachment bonds “our greatest protection against fear.” This is why it is harder to treat a child traumatized through chronic family abuse and neglect, compared to a single incident trauma on a child in a supportive family. And partly why parental separation from children in America’s migrant camps is so traumatic.
We are wired for connection through love. The matrix of bonding between infant and parent is an exquisitely sensitive dance. A mother and infant mutually influence each other’s emotional and physiological states. Neurobiological signals between a mother and child pass back and forth as fast as 1/300th of a second. One study showed that mothers and infants match heart rates as they respond to each other’s facial expressions (Heller, LaPierre, 2012). Healthy attachment between infant and parent establishes somatic and psychological coherence in the child. For example, when a father attunes to and soothes his infant, he regulates the baby’s nervous system. Disruption of attachment through chronic neglect/abuse or misattunement is traumatic. It impairs the child’s ability to develop self-regulation.
When a child is in distress from abuse/neglect, the sympathetic nervous system (SNS) activates, preparing for “fight or flight.” This would look like a baby starting to scream because no one has responded to their crying. The parasympathetic nervous system (PNS) slows us down and balances SNS activation. In on-going abuse, a child remains in chronic SNS hyper-arousal, along with chronically activated PNS (to balance the SNS). This results in a “freeze” state, like having your foot on the gas and brake at the same time. The intense energy of these activations remains undischarged in the nervous system, causing dysregulation. It is painful and in infants and children, it will lead to numbing themselves (cutting off from emotions, shame, denying needs). Tragically, in this way, a chronically abused child learns to forfeit their life essence in order to survive. Without appropriate regulation, traumatized children are unable to complete emotional and physical reactions that would otherwise move them out of the “freeze” response.
When PNS activation dominates, the “freeze” response looks more like collapse. This helps explain why parents often describe traumatized children in similar terms: collapsed, withdrawn, despondent. Children in this state tend to isolate. This is the most difficult type of trauma to treat. In addition, children tend to blame themselves for abuse. Shame from this, and the pain and rage of being abused by those they were supposed to trust most, only adds to feeling unsafe and hopeless. Children persistently treated with hostility or hatred learn to hate themselves and/or others. A parent’s self-loathing can be transmitted to the child. Self-loathing as self-directed aggression can become suicidal ideation. Outwardly, this can manifest as violence towards others. Abuse can also set a template for traumatic/toxic bonds, like “Stockholm Syndrome” in hostage situations. This information helps point us to how schools and parents can best assist with trauma healing.
Trauma Response in 5 Boulder Schools

Boulder Prep
Approximately 20 schools were contacted for this report; many did not reply. Schools that declined comment for this story include: St. Vrain Public School District, Boulder Country Day School, Dawson School, Sudbury School, and St. Vrain Community Montessori School. Charter Schools that participated are: Boulder Prep High School, Flagstaff Academy, and Peak to Peak. Private Schools included are: September School and Tara Performing Arts High School. All interviewed schools have observed an increase in trauma.
Boulder Prep High Charter School serves students labelled as “at risk.” Principal Lili Adeli exudes a palpable warmth when discussing her school. She paints a picture of an emotionally open, supportive environment that recruits its entire community to heal itself. Family-related traumas such as domestic violence are most common. Ms. Adeli does not believe in a blanket solution. Instead, Boulder Prep supports each of its 100 students as unique individuals. They initially get to know every student in an in-depth interview. Ms. Adeli emphasized that students in trauma need it addressed before they can be open to others and to learning. Personal connections with staff are encouraged in order to build trust. 100% of Boulder Prep’s staff are trauma-informed; according to PsychologyToday, “Trauma-informed care means treating a whole person, taking into account past trauma and the resulting coping mechanisms when attempting to understand behaviors and treat the” person. All teachers are trained to be able to show empathy and, when appropriate, redirect to learning. If further support is needed they can suggest referrals (including equine therapy at Medicine Horse), work with a student’s existing therapist and offer 6-8 week sabbaticals.
Boulder Prep does not practice shooting drills, and does not have a licensed therapist or school counselor. The school had a counselor before, but Ms. Adeli said it didn’t make much difference. She prefers its whole school approach, where students can be heard by any staff member. The transformations she’s seen are amazing and fulfilling. Still, Ms. Adeli lamented that the ones they cannot help are the most heartbreaking. It is the only school interviewed that has a therapy dog (named “Story”). It holds weekly “connection circles,” ensuring students’ voices are heard. The school also offers limited free therapy (thanks to a grant) and art therapy. The School Resource Officers’ (SROs) caring approach has broken down barriers. Not all schools are as fortunate. It really depends on the SRO, Ms. Adeli noted. In fact, while the National Association of School Resource Officers reports an unverified count of between 14,000-20,000 officers in 30 percent of the nation’s schools, “‘there is no evidence to show that expanding law enforcement by adding SROs actually results in safer schools,’ says Marc Schindler, head of the Justice Policy Institute,” according to NPR. Critics of SROs point out that “their presence creates unintended consequences like suspensions, expulsions and arrests — especially for students of color.”
Flagstaff Academy has 900 hundred students in pre-K to 8th grade. K-2 Principal Mrs. Gael Lester says Flagstaff now needs and is pursuing a whole school approach. Mrs. Lester observes increasing numbers of students with trauma and anxiety enrolling, and they also have fewer coping and social skills. She believes there are multiple factors, including fewer socialization skills from social media use, and fewer independent problem-solving skills caused byover-structured schedules including extra-curricular activities where children have little time without adults to intervene when problems arise. She cites neglect and physical abuse as the most commonly reported abuses.
Flagstaff holds “connection circles” to build community. It has two school counselors, and no licensed therapists or SROs. School counselors are “interim support.” They can suggest referrals, but can’t tell parents what to do. The school uses a “multi-tiered system of support” (MTSS), which includes administration, the dean, counselors, a special education facilitator and tier-2 interventionists. It individually approaches behavioral issues in students, and teaches non-harmful replacement behaviors.Flagstaff also has two Emergency Response Teams: one that trains for emergency incidents like fires, lockdowns, and evacuations. Another smaller team is trained through the Crisis Prevention Institute” (CPI). It has 7-8 staff members trained in-depth on de-escalation techniques. Mrs. Lester hasn’t noticed an overall negative impact from the school’s “lock-down and lock-out drills.”
Next year, Flagstaff will offer a socio-emotional learning curriculum (SEL). This curriculum teaches seven mindset principles to develop a success and happiness mindset. The idea is that the SEL will help students better handle trauma and still come out the other end shining.
Peak to Peak is a K-12 school, with approximately 1450 students. Melissa Christensen, Elementary School Principal, and Clara Quinlan, High School Assistant Principal, report more students experiencing trauma, including an increase in student disengagement. They also notice diversification in causes of trauma. Domestic violence is one of the most often reported abuses. The school has its own counseling team, which includes full time counselors, social workers, speech pathologists and special education teachers. Peak to Peak’s MTSS systematizes support when interventions are needed. The school does not have an SRO. Principals also monitor attendance. If attendance anomalies are observed, they talk to the student and can discover abuse that way.
The staff’s only trauma training is state-required mandatory reporter training, which, it should be noted, is not necessarily trauma-informed but a reporting mandate should abuse surface in the course of conversations. School counselors age-appropriately teach on subjects such as suicide prevention and drug abuse. They offer a 3rd grade sexual abuse awareness training, a 5th grade “kindness retreat” where they discuss bullying, and a 7th grade “courage retreat” where they discuss standing up for yourself. Asked if the resources for trauma met the needs at Peak to Peak, Ms. Christensen says, “sometimes.” There are cases where they choose to make referrals and they “can’t be everywhere all the time.”
Both Principals say students feel they can reach out to staff with concerns. This is likely facilitated by the impressive fact that every year, as their junior high students transition to high school, each student is individually discussed in a faculty-wide meeting.
According to Betsy Barricklow, Co-Director and Co-Founder of Tara Performing Arts High School, Tara is the only Waldorf school in America focused on performing arts with the intent to use it as a vehicle for adolescent development, not for producing performers. Tara emphasizes trust and communication for its 54 students. Ms. Barricklow described instances where students experience conflict during a play rehearsal. Taking students aside and working-out issues has had great results in addressing trauma. Ms. Barricklow also notices more students enrolling with trauma and anxiety. Family-related traumas are the most common, especially sexual abuse, emotional abuse, and trauma from viewing disturbing media/events on the internet.
Three other features are unique to Tara. One is its 100% substance-free requirement, in and out of school. Betsy says this is crucial for building trust and a safe environment. The second is its punishment-free, “restorative justice” approach to inappropriate behaviors. The school first asks students about such behaviors and help figure out the cause. Then it works with consequences. All staff are trained in “restorative justice” principles and receive trauma education in a mental health weekend course. The third feature is “sponsors,” who are two teachers that follow each entering class through all four years. This builds long-term trust and support. Tara doesn’t have a school counselor or licensed therapist, but offer referrals to trusted connections, including equine therapy. Responsive to student needs, the school invites licensed therapists to talk to student groups, as needed. Tara’s experiential wilderness trips are also very healing. Betsy emphasized the profound healing effect of the performing arts when intended for development, not production.

September School
September School is a private high school with 50 students and 2 full-time licensed therapists on staff. Kelly Molinet, Head and Executive Director of the school, says it is a relationship-based school where all teachers are trauma-informed. “Programs don’t change people, people change people,” Ms. Molinet stated. The school does not conduct “lock down and lock out” drills. Rather, mirroring Dr. van der Kolk’s sentiments, Ms. Molinet says its community’s sense of safety comes from their relationships. September’s adolescent-centered approach views each student as the author of his or her own experience. If a student was late several times, a teacher would approach them by saying: “This is the story I’m telling myself about your lateness. What am I getting wrong?” This respectful approach leads to students feeling heard and seen. It causes the teachers to self-reflect and check their bias. September is the only school that reports offering therapist-led support groups for parents. Ms. Molinet notes that parents don’t get a lot of support. These groups give parents a chance to vent, process trauma and find solutions.
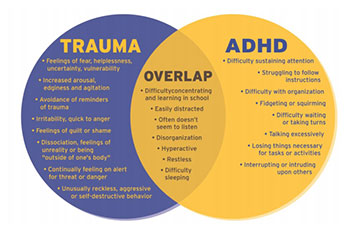
Family-related traumas (i.e. sexual abuse, divorce, rejection), sexual dating violence and bullying are most often reported at her school. MESA (Moving to End Sexual Assault) teaches there and its therapists lead various discussions throughout the year. For example, students may be invited to discuss their ADHD diagnosis, but say what they really feel is anxiety. Overlaps with trauma can be explored. There are community meetings several times a week so students can express themselves. Ms. Molinet is an advocate of staffing licensed therapists at schools. She says the confidentiality of children’s counseling is crucial for trust and healing, and is critical of school counselors who fully disclose student’s sessions to principals. While September School’s relationship-centered approach can be “messy,” Ms. Molinet is confident in its impact on trauma. Considering they have only had 4-5 CPS reports in the last four years and haven’t had an on-campus fight since the ‘70s, they seem to be onto something.

 Assessment: Strengths & Growth Areas for Schools
Assessment: Strengths & Growth Areas for Schools
Staff Training and School Involvement
Schools with a whole school, trauma-informed approach such as Boulder Prep, September and Tara seem to best support students. However, further trauma-specific staff training and education is imperative. State-required mandated reporter training alone (Peak to Peak’s only training) does not seem sufficient. Schools should be empowered by knowing the physiology of trauma and tools for nervous system regulation. I also believe child welfare organizations, law enforcement and other child professionals need to be trauma-informed. I spoke with Abi Blakeslee, PhD, who is a faculty member at the renowned Somatic Experiencing Trauma Institute and Legacy Faculty at the Ergos Levine Institute. She teaches nationally and internationally. She encouraged schools to see acting-out as dysregulation, and to see dysregulation as a natural, non-conscious, biological occurrence instead of seeing it as “bad,” “attention-seeking” or something to be controlled. She says the primary goal is to get children regulated first and then address behavior. This is key because the part of the brain needed to process a discussion on behavior will not optimally function with a dysregulated nervous system. Adding regulation techniques to MTSS interventions and Flagstaff’s SEL curriculum could be highly beneficial. Otherwise, for students with unresolved trauma, the SEL curriculum might be akin to building a skyscraper on an unsettled foundation.
Ms. Blakeslee strongly recommends parents and educators read “Trauma-Proofing Your Kids: A Parents’ Guide for Instilling Confidence, Joy and Resilience” (2008) by Peter A. Levine and Maggie Klein. Brad Kammer, LMFT, LPCC, is training director and senior staff at NARM. He believes educators also need to be informed that it is not the loud, aggressive students, but the quiet, withdrawn ones who are the most concerning. This indicates a collapsed “freeze” state. They are unlikely to approach teachers for help. Educators need to understand that a compliant, quiet appearance should not be mistaken for an absence of rage or pain. When they snap it can have the greatest consequences. He notes many of the school shooters fit this profile.
Mindset (Including Empathy and Communication)
There is a culture of institutional and adult narcissism that dehumanizes and dishonors children. Relations with children have been more about control than connection. Our mindset towards children needs to shift into one where we compassionately relate to them as unique beings, who are not there to do our bidding. Adults need to consider how they impact children. Our emotional literacy around “acting-out” needs to be upleveled. Mr. Kammer says our society is not set up for children. We objectify them and do things to them without their consent. We expect them to adapt to adults. Again, Ms. Blakeslee and Mr. Kammer emphasized being in relationship with children. Obtain consent. Ask what their behaviors mean. Many schools interviewed do this. I believe all schools need conscious languaging like the kind used by September School. One inspiring mindset resource is “The Conscious Parent: Transforming Ourselves, Empowering Our Children” (2010) by Dr. Shefali Tsabary.
Trauma–Specific Education and Support for Students
Trauma education and resilience-building classes for students (including age-appropriate nervous system education and regulation tools) would be empowering. Healthy social media use could also be taught. Regulation tools that integrate mind, body and spirit would benefit students. Trauma-specific student support groups could also be added. To my knowledge, no schools interviewed offer these.
Non Punishment
Tara High School’s rejection of punishment is exemplary. Understanding behavioral root causes is far more impactful. Mr. Kammer says punishment creates toxic dynamics of fear, shame and pain. The emphasis is again on compassionately getting in relationship with children. He recommends the documentary “Paper Tigers” (2015). It showcases the stunning results of an “at risk” high school that stopped punishing students.
Parental Support
September School’s provision of therapist-led parent support groups may prove to be an example for other schools. Aside from training schools, the greatest long-term influence in the child trauma epidemic lies in parental healing and education. In addition, Mr. Kammer recommended clinical support for families. Ms. Blakeslee urged the importance of having school counselors who are trained beyond talk therapy, who understand trauma’s physiology and help build resilience through body awareness.
There’s hope for healing. Human-made problems can be human unmade. Ms. Blakeslee says children with just a small amount of regulation go a long way. They are naturally able to connect to their inner world and know how to heal. Unlike adults, their minds don’t get in the way.
What You Can Do | Final Thoughts
There are many modalities that may help with trauma. Remember that what benefits one may not benefit another and to ask your doctor about them. Some possible modalities include: “Somatic Experiencing,” “NeuroAffective Relational Model,” Emotional Freedom Technique (EFT), Cognitive Behavioral Therapy (CBT), Eye Movement Desensitization and Reprocessing Therapy (EMDR), family therapy, animal-assisted therapies, therapeutic writing/art/dance/music, craniosacral therapy, “Theta Healing,” hypnotherapy, energy healing modalities (i.e. “Healing Touch” or “Pranic Healing”), yoga and meditation (specifically meditation that supports regulation). Healing should build regulation and resilience with a trustworthy, attuned, gentle trauma professional who understands how to guide the process. Ms. Blakeslee emphasized that the younger the child, the greater the need for sensitive, empathic attunement and mirroring by an adult.
Einstein said that a problem cannot be solved from the same level of consciousness that created it. Our current awareness has led us to a trauma epidemic, and we need higher consciousness to solve it. Nakia and Eduardo’s stories reveal deadly systemic failures, yet family abuses are the leading cause of child trauma. The greatest remedy for our child trauma epidemic lays in trauma-healing and educating parents and children, and trauma-educating schools and other child professionals. Also, to round out mind and body perspectives, I introduce a spiritual angle. According to Meg Blackburn Losey, MscD, PhD (2008), more children are being born highly sensitive and aware. They are higher vibrating souls, less inclined to blindly accept conditioning. They are called “indigo children,” “new children” and other monikers. Some say this explains increased youth ADHD diagnoses (Carroll, Tober, 1999). The predominant educational set-up simply doesn’t work for them. How is this connected to the trauma epidemic? In short, their sensitivity may be mirroring back adult trauma more vividly. It may sound “woo-woo” but that doesn’t mean it’s untrue. It’s possible these children are the higher consciousness that Einstein said we need.
While this may sound controversial, the need for healing and awareness in parents, parents-to-be and educators remains. Without your consciousness, your healing, without modelling this to youth, we will continue to engage in the emotional equivalent of toxic waste dumping upon our children. We will teach them inauthenticity through our own emotional repression. We will act from programs of dominance and subjugation, instead of fostering connection. We will see them through our unresolved trauma instead of as they are, and use them to dysfunctionally meet our needs, perpetuating unhealthy narcissism. We will deny our children’s pain and anger because we are overtaken by ours. In this way, we deprive children of the love they deserve.
Every parent was once a child who experienced the consequences of their parents’ unresolved trauma. So it has been for generations, and so it will accumulate until adults heroically take ownership for stopping the cycle of abuse. We need warriors willing to help end this social crisis. To do the life-giving work of transmuting the unconscious transmission and acting-out of intergenerational trauma. The power to do this is yours. It begins with making the choice.